Is it time to change the test for prostate cancer?
VIEWPOINT: ARU expert explains why digital rectal examinations are still important
By Stephen Hughes, Anglia Ruskin University
The finger-up-the-bottom examination for prostate cancer has been drawn into question. An international panel of experts recently suggested that so-called digital rectal examination for “active surveillance” should be replaced by MRI scans.
This news may be celebrated as the overcoming of an intrusive medical examination by the forward march of technology, but what exactly is a digital rectal examination (DRE) and what are the implications of replacing it?
The DRE involves a doctor examining a patient’s rectal wall by inserting a finger into the bottom. This gives doctors access to the prostate gland, helping them find signs of cancer. Before the prostate-specific antigen (PSA) test (from drawn blood) was introduced in 1986, the DRE was the only method of screening men for prostate cancer.
The DRE can also be used to detect other cancers, such as rectal cancer and anal cancer. It can be used to check for impacted stool in people with constipation, and, under certain circumstances which won’t be discussed further, foreign bodies.
It is also used in women to check for cancer, including the spread of ovarian cancer.
Done correctly, it shouldn’t be too uncomfortable. And privacy and good communication can go a long way in overcoming embarrassment.
All medical students are taught to do it and for generations have been told that when examining patients: “If you don’t put your finger in it, you may put your foot in it.”
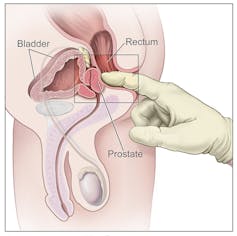
The walnut-sized prostate gland sits in the pelvis, surrounding the urethra as it leaves the bladder. Rather conveniently, it lies next to the rectum and is easily felt by the examining finger.
If it is inflamed, as in cases of prostatitis, it will be tender. And in benign prostate enlargement, which happens in middle age and causes the urinary stream to slow, the prostate gland will feel enlarged.
In cases of cancer of the prostate, the surface may be irregular and the texture firm to the touch. However, it is quite common for prostate cancer to be missed in the early stages of the disease.
The gloves are off
In the UK medical school system, great emphasis is quite rightly placed on learning good clinical skills. Over-reliance on technology is seen as potentially wasteful of scarce resources, and it would seem that patients like to think of their doctors as skilled diagnosticians. But there are times when technology is more accurate at finding disease – especially in its early stages.
Magnetic resonance imaging (MRI) provides detailed pictures of bodily structures. Unlike X-rays and CT scanning, it does not rely on ionising radiation (which is linked to an increased risk of cancer) and is thought to be safe. It is good at picking up early prostate cancer and for “surveillance” (monitoring the disease).
But MRI scans are expensive and the machines are bulky, power-hungry and usually confined to hospitals. This limits their use.
There is a blood test, the previously mentioned PSA test, which is used as a marker for diseases of the prostate, but it is not specific for cancer. When used in combination with the DRE, it helps to detect cases. But PSA levels become elevated after a DRE which makes the timing of testing awkward. It means blood needs to be drawn on a separate visit.
So what is the role of DRE in diagnosing prostate cancer? I believe it still has a place. Prostate cancer spreads easily to the bones, and it is not uncommon for undiagnosed prostate cancer to manifest as back pain when it has spread to the vertebrae. If this is suspected, then positive findings on rectal examination may lead to a more timely diagnosis and fewer delays in getting the correct treatment.
Gloves on again?
DRE performs rather better for rectal cancer. If the tumour is in a site accessible to the examiner’s finger, then up to 76% can be detected.
For constipation, the finding of impacted stool in the rectum can save the expense and radiation exposure of modern investigations, which have done away with X-rays of the abdomen in favour of radiation-intensive CT scans.
Has the rectal examination had its day? I think not. It’s a cheap examination that yields useful information when used and interpreted correctly.![]()
Stephen Hughes, Senior Lecturer in Medicine, Anglia Ruskin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
The opinions expressed in VIEWPOINT articles are those of the author(s) and do not necessarily reflect the views of ARU.
If you wish to republish this article, please follow these guidelines: https://theconversation.com/uk/republishing-guidelines